
")


From medical language to medical codingPersonal
Ana Luisa Villanueva
Chief Medical Officer, Life, Health & Accidents
MAPFRE RE
Madrid - Spain
The origin of Medical Coding

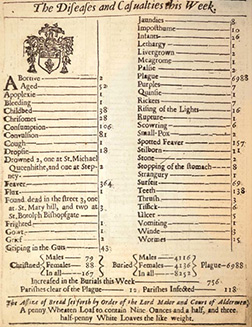






Among the many concerns of human beings, death has always been present through disease. There was not only evidence of its presence in Arts, thought artistic representations, but in writing. The need to communicate the cause of death is obvious in the Middle Ages. In 1348, Boccaccio in his book, The Decameron, refers to death caused by bubonic plague, called Black Death. Later in 1629, local Parish Clerks in various geographical areas of London collected the information concerning births and deaths in the parish and every December, each diocese made it public. These were known as «The London Bills of Mortality». They are the first known mortality statistics in the History of Medicine. These clerks lacked of any medical knowledge, deaths had descriptions like griping in the guts, teeth or eaten by lice.
In 1665, John Graunt, a London merchant, published «Reflections on the weekly bills of mortality». Its central theme was that deaths from plague needed to be examined in the context of all the other causes of mortality in order to understand the effects of all diseases. The sixty disease categories in the Bills constitute the first systematic attempt to analyze the incidence of disease. Nosology arises as the branch of medicine that deals with classification of diseases.
During the eighteen century, additional classifications were authored by Linnaeus in Sweden (Genera Morborum, 1763), Bossier de Lacroix in France (Nosologia Methodica, 1785) and Cullen in Scotland (Synopsis Nosologic Methodicae, 1785).
The first medical statistician for the General Register Office of England, Dr. William Farr, revamped the Cullen disease classification to standardize the terminology and utilize the first primary disease instead of complications. Farr incorporated additional data, enabling reporting and analysis of factor such as occupation and its effect on cause of death.
The need for a uniform classification of causes of death was recognized at the International Statistical Congress convened in Brussels in 1853. From here came out the first of 138 diseases, which was adopted in 1864 and revised at four subsequent Congresses.
Nosology arises as the branch of medicine that deals with classification of diseases
In 1839, the International Statistical Institute adopted a revised list of diseases prepared by Jacques Bertillon, chief statistician of the City of Paris. Known as the Bertillon Classification, it was the first standard system implemented internationally. The American Public Health Association recommended its use in the United States, Canada and Mexico by 1898. 26 countries adopted the Bertillon Classification in 1900 which had subsequent revisions through 1920.
After Bertillon’s death in 1922, interest grew in using the classification to categorize, not only causes of mortality, but also causes of morbidity. Morbidity refers to a health state or the incidence of a disease in a population. As early as 1928, The Health Organization of the League of Nations published a study defining how the death classifications scheme would need to be expanded to accommodate disease tabulation.
In short, any disease, symptom, sign or medical or surgical procedure can be identified by codes, thus providing data storage, safe data transfer and statistics.
Codes, language and content
Medical language is one of the least known languages among the world population. Only medical and healthcare staffs are familiar with this specific jargon of the human body. For us doctors, it is much easier to talk to patients in these terms to properly express situations that have no clear translation into popular wording.
What matters is not the information itself but what we can do with it: key words to identify texts, numeric data to enable big statistical analysis to improve management, payments, performance or any work-in-process, in short «Big Data».

What is Big Data?
Every day, we create 2.5 quintillion bytes of data - so much that 90% of the data in the world today has been created in the last two years alone. This data comes from everywhere: sensors used to gather climate information, posts to social media sites, digital pictures and videos, purchase transaction records, and cell phone GPS signals to name a few. This data is Big Data.
Big Data spans three dimensions: Volume, Velocity and Variety.
Volume: Enterprises are awash with ever-growing data of all types, easily amassing terabytes -even petabytes- of information.
Velocity: Sometimes 2 minutes is too late. For time-sensitive processes such as catching fraud, Big Data must be used as it streams into your enterprise in order to maximise its value.
Variety: Big Data is any type of data - structured and unstructured data such as text, sensor data, audio, video, click streams, log files and more. New insights are found when analysing these data types together.
Big Data is more than simply a matter of size; it is an opportunity to find insights in new and emerging types of data and content, to make your business more agile, and to answer questions that were previously considered beyond your reach. Until now, there was no practical way to harvest this opportunity.
Source: IBM
http://www-03.ibm.com/software/products/en/category/SWP10
From Paper Medical Records to Electronic Health Record
In recent years, thanks to the widespread use of computer technology, a large amount of text information has been stored, written in normal language, unstructured, making analysis very complex or impossible in some cases, as expert system or analysis software do not understand it.
Patient’s medical record is the main source of information, not only to know about the health state but to manage it. Doctors write their impressions and comments on patients in their own language, easy for them to understand, but hard for analysis on characteristics or condition present in their patients.
Critics of this paper model suggest that the available information may be incomplete, illegible, damaged by external elements such as water, food or fire. It may as well lack of confidentiality due to circulation from hand to hand, with the risk of losing any included document or lack of imaging due to the inability to store them in paper.
We must not forget that medical records are a scientific and legal document:
- Scientific as they collect information on the health state of the individual, providing relevant data having multiple applications.
- Legal in different areas as forensic, criminal arbitrage, bodily damage and personal insurance. Therefore, it must be true, clearly written, in chronological order, including relevant information such as physical exam, diagnose, therapy, complications, indications on lifestyle and expected developments.
Therefore, medical records should have information easy to retrieve.
Information systems
Information systems enter healthcare in the fifties developing medical software to help mainly the administration and finance department to translate medical procedures and bill them. This is one of the main reasons for the United States to develop the adapted ICD-8 and procedural terminology. The era of medical billing starts.
Medical coding and billing represent a key step in the healthcare industry. They are the link between healthcare and its economical value. Any type of care due to a disease is formulated into a series of codes showing the procedures used and their cost. This way a detailed invoice is issued, valid in both public and private/insurance environments.
CPT or Current Procedure Terminology is widely used in insurance, mainly in English speaking countries. It is a set of codes developed and constantly maintained by the American Medical Association
The CPT or Current Procedure Terminology is a set of codes developed and constantly maintained by the American Medical Association, AMA. The code set describes medical, surgical, and diagnostic services and is designed to communicate uniform information about medical services and procedures among physicians, coders, patients, accreditation organizations, and payers for administrative, financial, and analytical purposes. This unified coding enables standardization of administrative, financial and analytical tasks. CPT coding is widely used in insurance, mainly in English speaking countries. Some companies have developed their own coding as there was no approved code set.
Healthcare Information Management in Insurance
Insurance is based on risk factors analysis to develop different products. Information technologies help actuaries developing models using a great number of variables.
Diagnosis has a major role in medicine. Clinicians rely on it for analysis, decision-making and performance. Lately, the structure and formulation of diagnosis has undergone major changes to better meet its goal, particularly regarding data confidentiality, process and transmission. Part of the new challenges are related to the introduction of this International Classification of Diseases.
Information systems enter healthcare in the fifties. The era of medical billing starts
The health status of the individual is basic to determine the risk to insure. Health questionnaires are developed by insurers for the applicant to answer questions on their health.
Coding of the disclosed conditions or procedures enables using data to/for:
- Study portfolio profiles, identifying which conditions or procedures are more common by sex, age, geographical distribution and lifestyle. For example: diabetic endemic populations.
- Product design to meet buyer’s needs. For example, saving products vs. risk products or specific health insurance products for certain conditions.
- Cost analysis, studying the cost of medical tests required to have a diagnosis.
- Epidemiological studies to understand how diseases behave.
- Analysis of new diseases that formerly were not a threat for the individual or are caused by a change in lifestyle.
- Development of predictive models related to health which enables prediction of future behaviour. Mortality and morbidity related to lifestyle and economical status or other patterns of behaviour depending on the available information.
Management of health information in an economic environment
Decisions made by health administrators, either public or private, highly depend on the quality of the produced information, hence the importance of adequate completion of files and careful processing of information, verifying full covered service and minimizing mistakes in coding and data capture.
Medical coding and billing represent a key step in healthcare. They are the link between healthcare and its economical value
The lack of uniformity on code systems can cause the same condition to be encoded in different ways, modifying mortality statistics and hindering the cost analysis on diagnosis and treatment.
New management systems enable the integration of costs related to health care, hospital care, surgical procedures, diagnostic imaging and laboratory testing and are used both nationally and internationally.
In insurance, choosing the right coding systems will affect the use and application of the information.
- Immediate payment of services. Insurer-hospital / health provider / physician.
- Claims payment to third parties.
- Updating Health care cost.
- Change in protocols.
- Hospital inventory management.
- Productivity ratios.
| Current Coding | |
|---|---|
| 1949 | International Conference for the Sixth Decennial Revision of the World
Health Organization, convened in Paris. The «International Classification of Disease, Injuries and Causes of Death», called ICD (International Disease Classification) is created. An extensive list of mortality and morbidity statistics was adopted and endorsed the international rules for selecting the underlying causes of death. From now on, the use of ICD was extended to tabulation, registration and use of data for the planning and evaluation of Health Services. The purpose of the IDC and the WHO is to promote the international agreement in the collection, classification, processing and presentation of mortality and morbidity statistics. |
| 1900 | ICD-1. The Unites States of America implemented ICD-1 in 1900. |
| 1900-1968 | ICD-2 to ICD-7. Successive revisions. It is used not only to classify the causes of death disease but to index diseases. |
| 1968 | ICD-8. The United Sates developed their own version called ICDA-8 or International Classification of Disease Adapted, due to disagreements with the international version. |
| 1975 | In parallel to ICD-9, the International Classification of Procedures in Medicine ICPM was developed and published in 1978. Divided into fascicles (bundles or groups of subjects), each issue contains procedures laboratory, radiology, surgery, therapies and diagnostic procedures. Many countries have adapted and translated some or all of the CIPM. |
| 1976 | ICD-9. The Ninth Revision was attended by delegations from 46 countries,
who debated on a more detailed classification, required by those countries using ICD for evaluation of medical care and for payment purposes. Its
implementation was effective January 1, 1979.
The United States of America adopted a modified version called ICD-9-CM, International Classification of Diseases, Clinical Modification. This CIE-9-MC has had many amendments over the years to adjust to changes in Healthcare Management, including codes for new diseases such as AIDS and related conditions, a tick-borne condition known as Lyme disease, Kaposi’s sarcoma, toxic oil syndrome, HPV Human papillomavirus, morbid obesity, necrotizing fasciitis, toxic shock syndrome and SARS. |
| 1983 | ICD-10. The new revision was endorsed by the Forty-third World Health
Assembly in May 1990. The latest version came into use in 1994. The classification system allows more than 155,000 different codes and permits tracking of many new diagnoses and procedures. |
| 2013 | CIE-11. The World Health Organization is currently revising the latest version.
The development is taking place on an internet-based workspace, called iCAT
(Internet Collaborative Authoring Tool) Platform, somewhat similar to a wiki –
yet it requires more structure and peer review process. The WHO collaborates through this platform with all interested parties. The final new version is expected to be submitted for official endorsement by 2017. The information in ICD-11 will be more structured, unlike version 10, which only refers to the name of the disease, now each disease will have specific definitions. |
| The ICD is translated into forty one languages and is available on-line. | |
There is a lack of uniformity in procedural terminology and medical coding
In some countries, such as the United States, physicians do not receive their fees from insurers if they do not send all required paperwork including medical and CPT codes.
Nowadays the use of on-line billing models is widespread. The chip card in healthcare identification cards has different functions:
- Report to clinics and physician that insured from a certain company is up to date with premium payments and /or has coverage for service.
- Accelerate invoicing through an on-line transaction so procedures are automatically written on company accounts.
The purpose of the International Classification of Diseases, ICD, and the WHO is to promote the international agreement in the collection, classification, processing and presentation of mortality and morbidity statistics
Although this system has greatly improved invoicing, there is still a long way to go. There is a lack of uniformity in procedural terminology and medical coding.
As insurance companies include these concepts in their business models, products will be more competitive and allow a bespoken design according to end user needs.

| Chapter | Blocks | Title |
|---|---|---|
| I | A00-B99 | Certain infectious and parasitic diseases. |
| II | C00-D48 | Neoplasms. |
| III | D50-D89 | Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism. |
| IV | E00-E90 | Endocrine, nutritional and metabolic diseases. |
| V | F00-F99 | Mental and behavioural disorders. |
| VI | G00-G99 | Diseases of the nervous system. |
| VII | H00-H59 | Diseases of the eye and adnexa. |
| VIII | H60-H95 | Diseases of the ear and mastoid process. |
| IX | I00-I99 | Diseases of the circulatory system. |
| X | J00-J99 | Diseases of the respiratory system. |
| XI | K00-K93 | Diseases of the digestive system. |
| XII | L00-L99 | Diseases of the skin and subcutaneous tissue. |
| XIII | M00-M99 | Diseases of the musculoskeletal system and connective tissue. |
| XIV | N00-N99 | Diseases of the genitourinary system. |
| XV | O00-O99 | Pregnancy, childbirth and the puerperium. |
| XVI | P00-P96 | Certain conditions originating in the perinatal period. |
| XVII | Q00-Q99 | Congenital malformations, deformations and chromosomal abnormalities. |
| XVIII | R00-R99 | Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified. |
| XIX | S00-T98 | Injury, poisoning and certain other consequences of external causes. |
| XX | V01-Y99 | External causes of morbidity and mortality. |
| XXI | Z00-Z99 | Factors influencing health status and contact with health services. |
| XXII | U00-U99 | Codes for special purposes. |
|

Conclusions
In short, any disease, symptom, sign or medical or surgical procedure can be identified by codes, thus providing data storage, safe data transfer and statistics
Information technology has become an important part in the modern concept of Public Health and healthcare policy in each country. This resource can help healthcare institutions to plan their strategies to promote health and communicate related key messages.
Applying information technology to Health Science enables:
- The use of expert systems as structuring knowledge models or educational models.
- The analysis of large amounts of data in an homogeneous and safe environmental way, useful to both public sector and insurance.
- Integration of further evidence, including both lab and imaging testing.
- Improving service delivery through a more efficient service and financial management.
- Development of mathematical models for physiopathological process to relate parameters to a model and study the effect of modification of the existing variables.
- Medical training with simulators reproducing patient behaviour to allow learning patients care.
- The development of laboratory and high precision surgical techniques to analyze, remove or provide treatment in areas otherwise very difficult or impossible to access.
References
- Guide to State Implementation of ICD-10 for Mortality. National Center for Health Statistics website 1998.
- History of the development of the ICD.
Available at:
www.who.int - J.J. O’Connor and E.F. Robertson. Adolphe-Louise
Jacques Bertillon. Copyright 2009, University
of St. Andrews, School of Mathematics and
Statistics.
Available at:
www.anthemcollege.edu - Medical coding in history.
www.jblearning.com - Replacing ICD-9-CM with ICD-10-CM and
ICD-10-PCS: Challenges, Estimated Costs
and Potential Benefits. 2003. Robert E. Nolan
Company website.
Available at:
http://www.renolan.com - Scientific Data Documentation International Classification of Diseases-9 (1975). CDC Wonder Website.